
Lower limb injuries in breaststroke swimmers: Epidemiology and common conditions
icon
We all know that shoulder pain is by far the most prevalent injury in the competitive swimming population, with prevalence reported between 40% and 90%, depending on what you read. Considering that the upper limbs provide up to 80% of forward propulsion in freestyle, backstroke and butterfly, it is no wonder that injury to the shoulder proves costly to the competitive swimmer.
Often overlooked though, is our subgroup of breaststroke specialists who rely more on the powerful propulsion of the breaststroke kick, and suffer a high prevalence of associated hip, groin and knee pain.
Research in the area of breaststroke related injuries is scarce and of poor methodological quality. The majority of the research has consisted of retrospective questionnaires or surveys of competitive swimmers, related to quantifying injury epidemiology, and identifying risk factors associated with injuries.
Overall prevalence of knee pain in U.S college swimming has been reported as around 30-40%, but when looking at breaststroke specialists only, the prevalence is actually be closer to 85%. The incidence of groin pain has been reported as 43% in breaststrokers, significantly higher that in individual medley swimmers (22%) and non-breaststroke, non-IM swimmers (6%).
Many breaststrokers suffering abdominal, hip, groin or knee pain, continue to train without reporting symptoms or seeking treatment, resulting in chronic injury conditions, as well as costly and lengthy rehabilitation.
Breaststrokers with kick related injuries often fly under the injury prevention and management radar!
In this three part blog series, we will discuss common lower limb injuries in breaststroke swimmers, their risk factors, and specific injury prevention strategies.
COMMON INJURIES
Lower limb injury arising from breaststroke kick is often of gradual onset, rarely the result of an acute injury episode, and as such is often termed an overuse injury.
Lower limb injury in breaststroke is not always completely debilitating, and many swimmers may be able to continue to train in some capacity while managing their symptoms. Unfortunately this means that many breaststroke related injuries go untreated, and become chronic and recurrent.
The most common lower limb injuries that we see in breaststrokers are related to knee pain and groin pain:
Knee pain
Knee pain in breaststrokers has varied presentations, but manifests most commonly as anteromedial knee pain (pain at the front, inside edge of the knee).
Knee pain in breaststroke can come from a variety of anatomical structures, including:
Patellofemoral joint (Patellofemoral joint pain syndrome)Medial plica (Medial Plica syndrome)
Medial collateral ligament (MCL Sprain)
Infrapatella fat pad
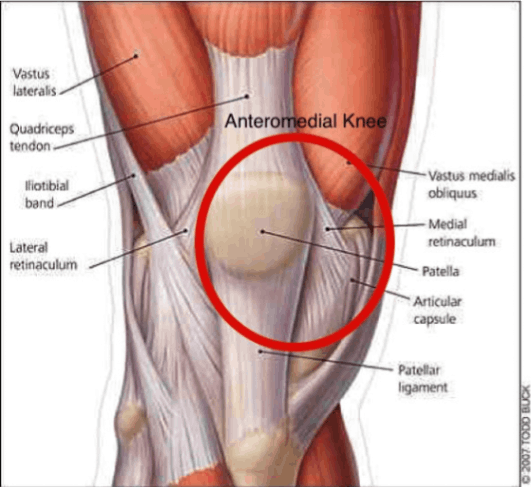
While there are some congenital structural abnormalities around the knee and kneecap (patella) that might predispose a breaststroker to knee pain (e.g.: trochlear dysplasia or patella alta), it is most often a mechanical dysfunction in which unbalanced stress is placed on various areas of the anteromedial knee joint and multiplied by high load and high repetition, resulting in pain and dysfunction. Although the specific anatomical structures that become painful will vary slightly between individuals, the drivers for the problem are often similar.
In most cases, there is no structural damage to the knee, and functional changes are often reversible with quality rehabilitation and implementation of load management strategies.
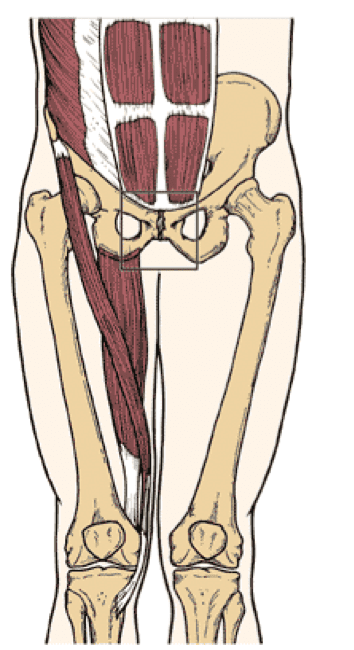
Groin pain
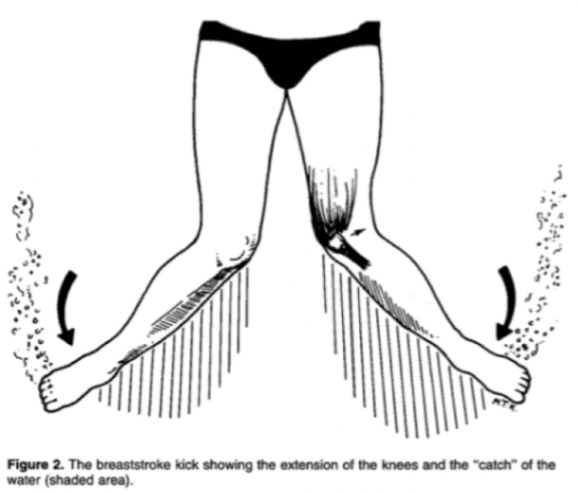
The groin is an anatomically complex junction of major muscle groups, including the hip adductors, hip flexors and abdominals, all of which are primary force producers in the breaststroke kick, and fall under considerable stress during breaststroke swimming.
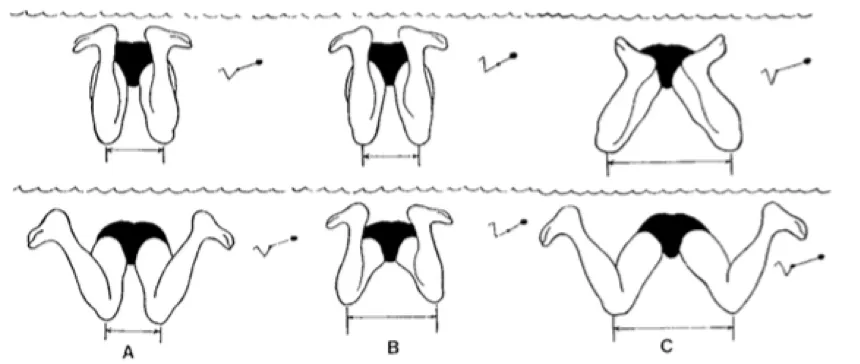
The wider that the knees and feet travel from the midline in the propulsive phase of the breaststroke kick, the more the groin load is increased. This is one of the reasons why the narrow knee “whip kick” is advocated:
Groin pain in breaststrokers may present as an acute or sudden strain of one or more of the contributing muscle groups or their tendons, or develop more chronically as a result of repetitive overload and stress on a dysfunctional anatomical system.
We often triage groin injury to its primary driver, although it’s important to remember that it is possible to have multiple painful pathologies occurring concurrently at the groin.
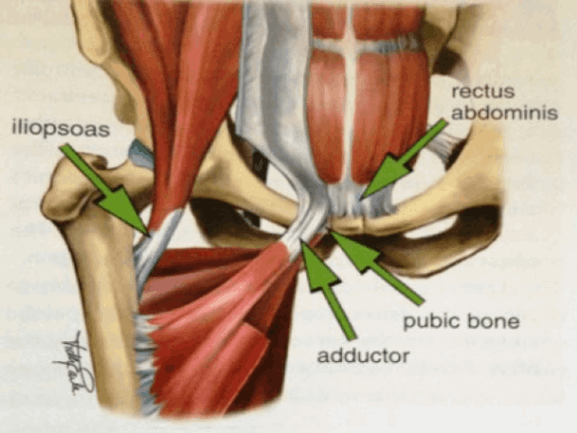
There are three primary drivers of groin pain:
a) Adductor related groin pain
This refers to pain coming from the inner thigh muscles that act to squeeze the legs together in the propulsive phase of the breaststroke kick and often occurs at the tendon portion of the muscle (musculotendinous junction or tendon insertion).
b) Hip Flexor related groin pain (iliopsoas)
This refers to groin pain coming from the hip flexor muscles, which are used during the recovery and set up phases of the breaststroke kick. The hip flexor muscles can often be the compensators for deficiencies in core or gluteal strength, and often become overloaded under fatigue.
c) Abdominal related groin pain (Rectus Abdominis)
Groin pain may also come from strain or hypertonia of the rectus abdominis at its insertion to the pelvis. The abdominals are likely to function during multiple phases of the breaststroke kick and provide stability of the pelvis and body position as well as a splint for the production of lower limb power.
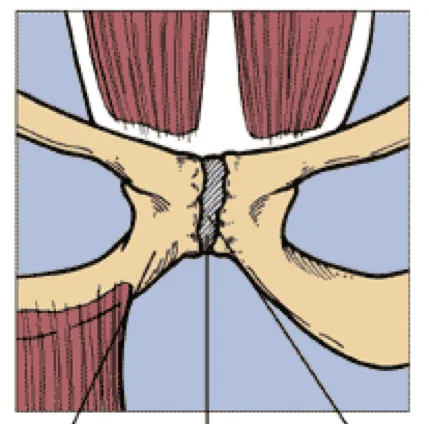
Pubic bone Overload (“Osteitis Pubis” or “Traction Apophysitis”)
This refers to a difficult groin pain condition that can develop from recurrent or chronic groin stress coming from one or a combination of the major muscle groups attaching to the pubic bone.
The specific pathologies that can occur at this site may differ for each person, depending on their age and contributing factors. This means that it can be difficult to manage and often requires a period of complete rest before progressive return to training as well as patience with consistent and structured Physiotherapy rehabilitation.
I hope part I of this blog has given you an introduction to the epidemiology and nature of the common breaststroke related lower limb injuries. In Part II, we will discuss risk factors for these breaststroke related lower limb injuries in swimmers.
Book an appointment at Coast Sport by calling (02) 4356 2588 or book online via the button below.
Thanks to Coast Sport Physiotherapist Brett for preparing this blog. You can find out more about Brett here.


