
icon
In Part I of this blog, we discussed the epidemiology of breaststroke related injury, as well as the common presentations of knee, abdominal, hip and groin pain associated with breaststroke kick. If you haven’t already, you can read part 1 here.
Identifying risk factors for injury allows us to target our injury prevention strategies. From the available research, and our clinical experience, we can suggest that risk factors for lower limb injury in breaststroke are likely to include:
1) Age
Multiple studies across various sports have reported that the older you are, the more likely you are to get injured. This has been reported specifically for groin and knee pain in breaststrokers, with increases in injury frequency reported in breaststrokers over the age of 16. Age is an uncontrollable risk factor, but awareness of this means paying more attention to controllable risk factors.
2) Training age
The more years you have been competing as a competitive swimmer, the more likely you are to sustain injury. A study reported those breaststrokers with a training history of >9 years were associated with more frequent breaststroke related knee pain. This might be related to the cumulative effect of repetitive stress on the hip and knee over years of training.
3) Warm-up
One study correlated reduced warm up distances with increased breaststroke injury incidence in college swimmers in the USA. Those performing less than average 900m warm up were associated with significantly more frequent knee pain episodes. Specific warm up volumes should be tailored to individual requirements by the coach and the age, training history, and ability of the swimmer needs to be considered when prescribing warm up.
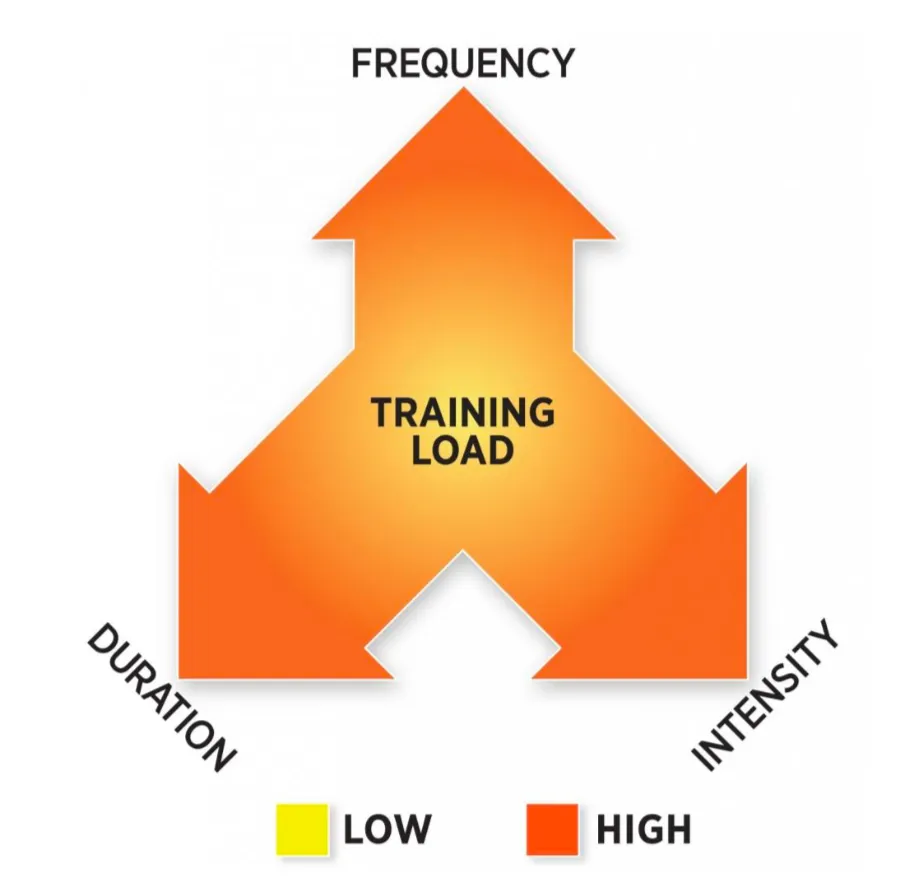
4) Breaststroke training load
There are two concepts to understand here: Absolute Training Load and Training Stress Balance (TSB).
Absolute Training Load:
This refers to the total amount of breaststroke training over a given time period, that an individual can handle before they get injured. No research has been published related specifically to absolute breaststroke training loads although it is likely that an individualized ‘ceiling’ exists for absolute training load vs. injury risk. It may be advisable that coaches and athletes begin monitoring breaststroke training load specifically so that trends and individualized tolerance profiles can be identified.
Training Stress Balance (TSB):
Sudden (acute) large changes in training load are a risk factor for injury. This has been shown in the literature across other sports, and is currently being investigated for swimming. TSB indicates the magnitude of acute change in training load:
TSB = acute load / chronic load
Where:
Acute load = training performed this week
Chronic load = average weekly training for the last 4-weeks
Current evidence suggests that training programs should maintain a TSB of less than 150% to reduce injury risk.
This means that training should be consistent to minimize injury risk. Plan your training so that you avoid long breaks as well as sudden spikes in load. Changes in training loads (whether increasing OR decreasing) should be progressive. Research across other sports shows that acute spikes in training load can result in elevated injury risk for 4-6 weeks following the acute load increase.
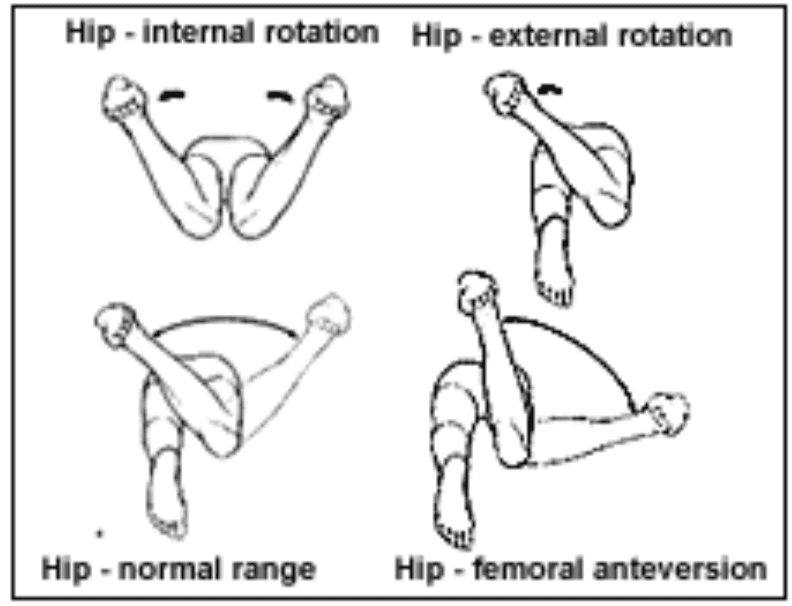
5) Technique
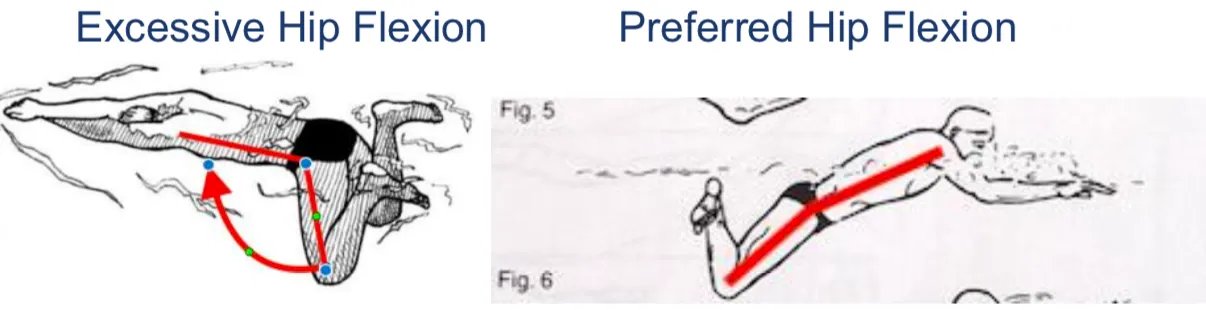
Incorrect technique can result in increased stress on particular anatomical structures (knee and groin), leading to pain or mechanical failure over time. Common technical faults in breaststroke kick include:
Lack of hip internal rotation causing wide knees (Hip abduction) and increased groin load. Lack of foot turn out (Tibial Torsion), increasing rotational load through the knee and hip and reducing propulsion.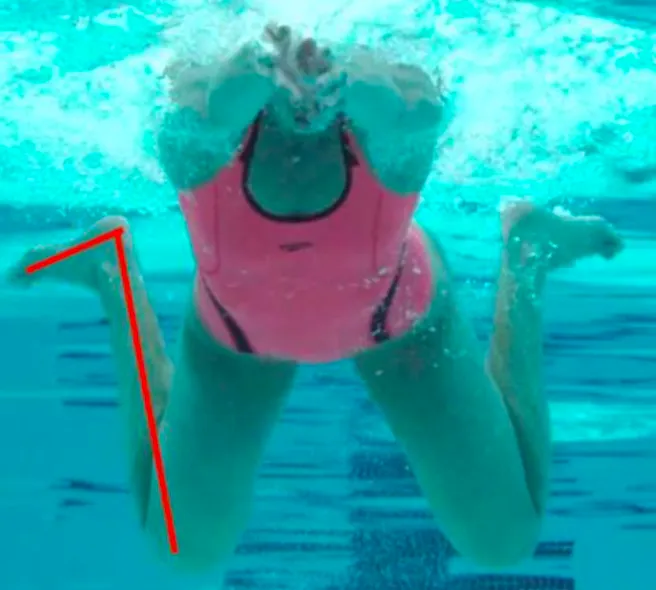
6) Joint range of motion
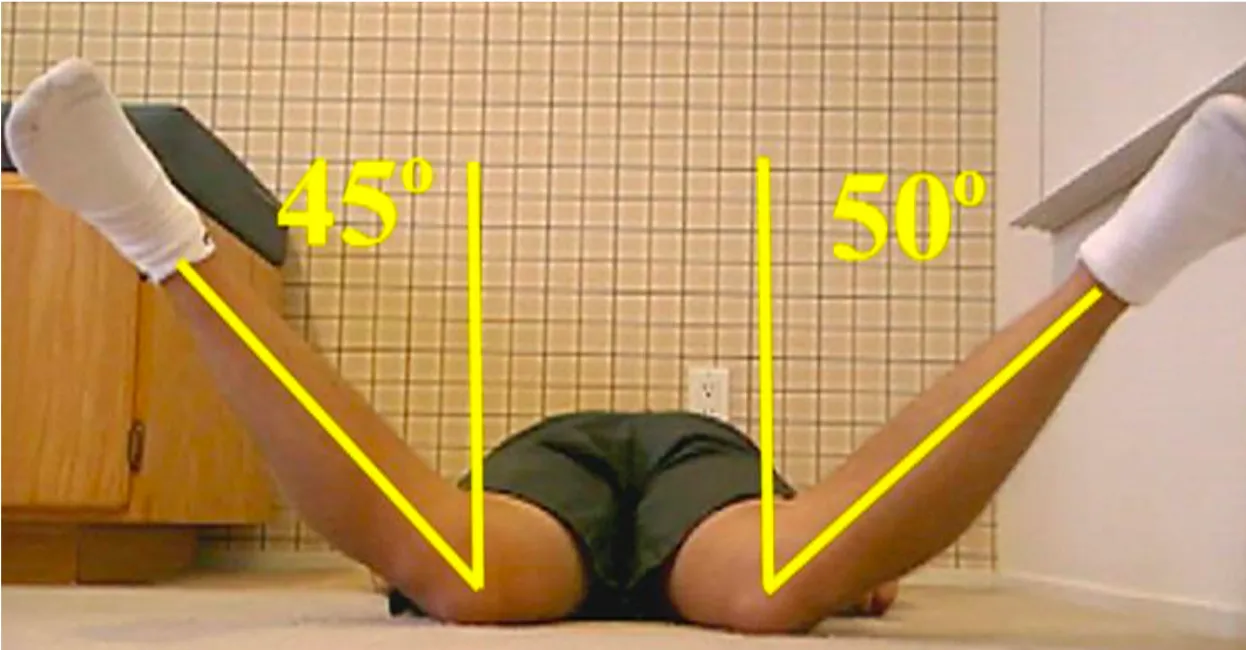
Adequate hip internal rotation and tibial torsion range of motion are essential to achieve the body position to kick with correct technique in breaststroke. Physiotherapists can accurately assess this mobility and prescribe interventions to improve them. As a guide, hip internal rotation is ideally around 40°, and tibial torsion around 50°. There is some room for movement here, as we generally consider the following sum an important indicator of breaststroke specific lower limb mobility:
Hip internal rotation ROM + tibial torsion ROM ≈ 90°
Measurement of prone hip internal rotation:
Measurement of seated tibial torsion:

Improving hip movements will minimize stress on the knees. Ensuring adequate internal and external hip rotation will transfer the rotary stress of the breaststroke kick away from the knees and into the hips, which are better suited to handle rotary forces.
7) Hip strength
Adequate strength is required to support the knee and hip joints and soft tissues under the load of the breaststroke kick.
Current research is investigating the responsibility of hip abduction (pushing out) vs. hip adduction (pushing in) strength and hip internal rotation vs. hip external rotation strength in relation to lower limb injury related to breaststroke.
These strengths are specifically relevant to the breaststroke kick and have been shown to be relevant in other sports in relation to risk of lower limb injury.
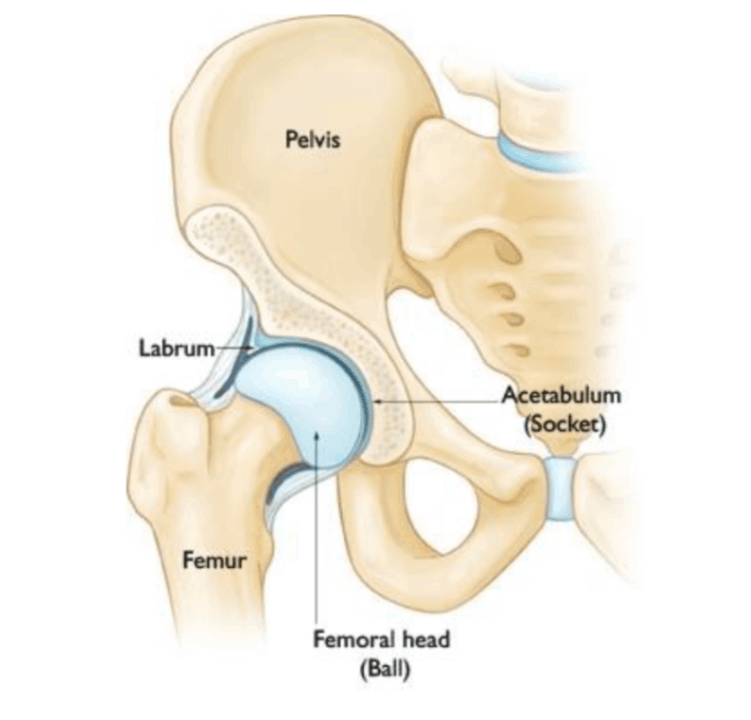
8) Bone structure
There has been some suggestion that bony structure of the pelvis, hip joint and femur may predispose an individual to success or failure in breaststroke. The bone structure may influence the risk of injury, as well as performance.
This is due to the influence of bony structure on the availability of breaststroke specific hip range of motion, particularly in relation to the important internal and external rotation movements required during breaststroke kick.
Common bony irregularities that may influence hip mobility in breaststroke include:
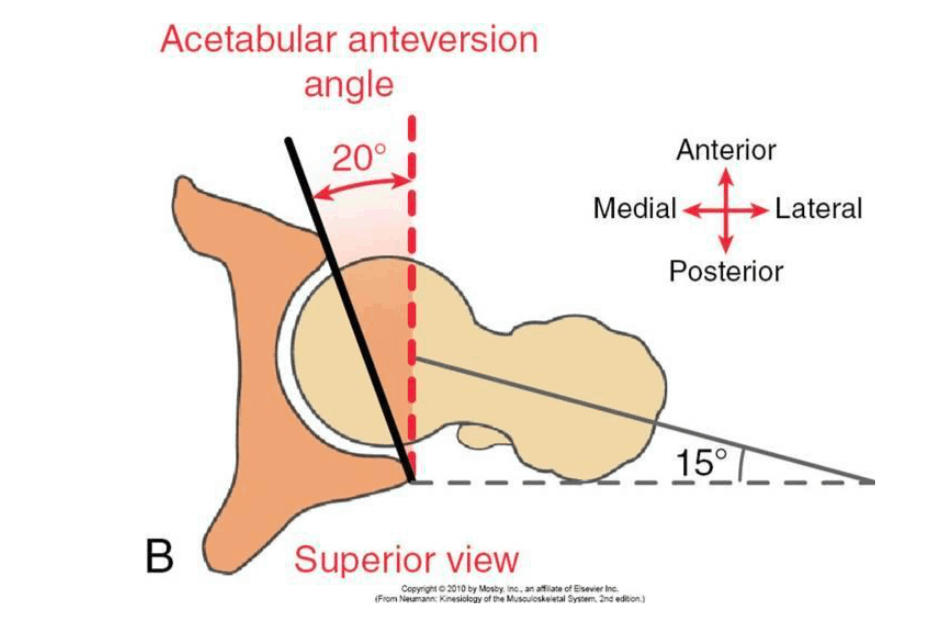
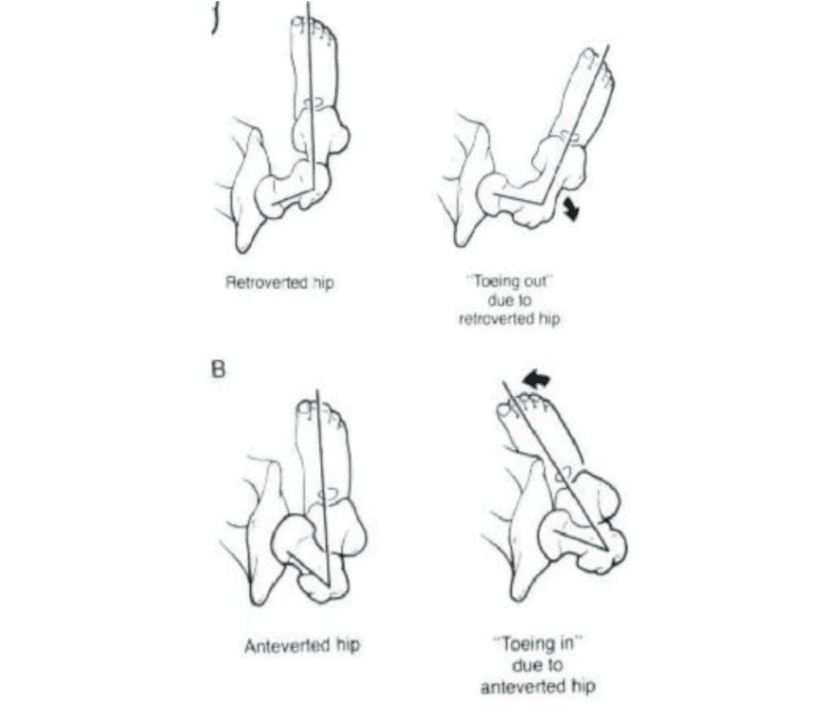
Femoral-Hip retroversion/anteversion:
This refers to either the femoral head (ball) or the acetabulum (socket) being shaped to face forward or backward. It is usually a congenital or developmental abnormality and is diagnosed through XRAY. Acetabular anterversion will bias the individual to more hip internal rotation.
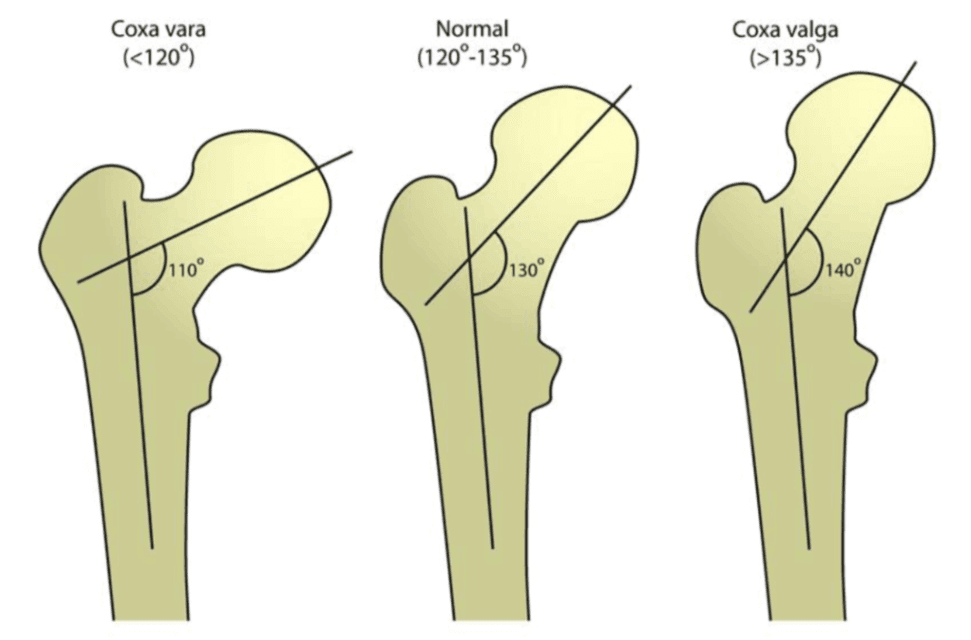
Coxa Vara or Coxa Valga:
This refers to the angle of the femoral head (ball) in relation to the femoral shaft in the frontal plane and is diagnosed through XRAY. Coxa valga may bias the swimmer toward having more hip external rotation range of motion while coxa vara may bias the swimmer toward more internal rotation range of motion.
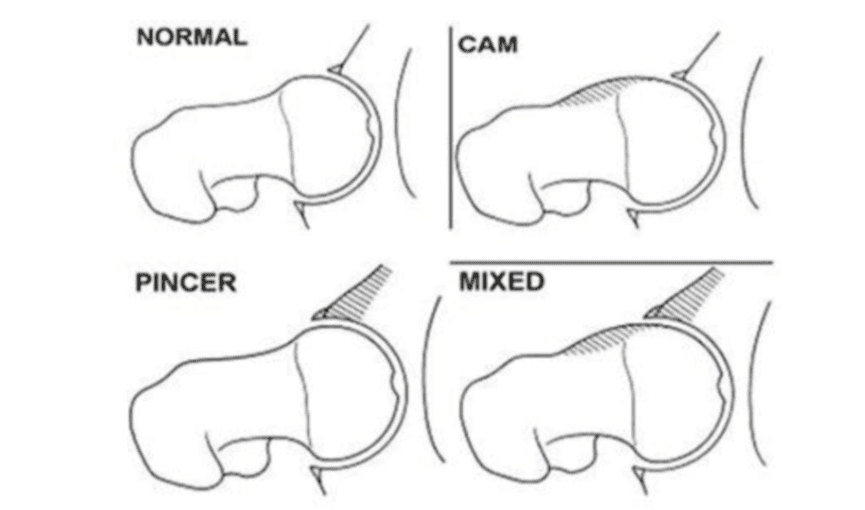
Femoroacetabular impingement (FAI)
This is the formation of extra bone around the hip joint, forming a physical block to mobility. FAI is a condition that may develop with age or in response to bony stress placed around the hip joint. Abnormalities of the acetabulum or femur like anteversion/retroversion or coxa vara/valga may predispose an individual to developing FAI.
Most bony irregularities at the hip in breaststrokers are successfully managed through Physiotherapy and optimization of the controllable risk factors, including range of motion, strength, neuromuscular control and load management.
Bony irregularities that do not respond to conservative management and continue to cause disabling pain and affect daily living may be addressed surgically.
It is important to remember that bone changes with growth and this continues into the late teenage years. This means that joint measurements in young swimmers are not permanent, and certainly not an absolute determinant of breaststroke success or failure. Your physiotherapist can help you monitor joint changes with growth and their effect on your mobility.
Summary
It is important to remember that there are many ways to skin the breaststroke cat. Ultimately we see eight swimmers in an Olympic final using vastly different strategies, based on their individual strengths and weaknesses, to achieve a result that might be within 0.2 seconds across the field.
It is the careful management of the risk factors and individuals advantageous and disadvantageous anatomical and physiological adaptations that can avoid injury and produce a successful breaststroker.
Physiotherapists are experts in the assessment of risk factors, as well as the prescription of prevention programs to reduce your injury risk. We recommend that all breaststroke swimmers should be screened for injury risk and the provision of an injury prevention program.
In part III of this blog we will discuss lower limb injury prevention strategies for breaststrokers.
At Coast Sport we can help with swimming injuries, screenings and strength and conditioning. Book an appointment by calling 4356 2588 or book online via the button below.
Thanks to Coast Sport Physiotherapist Brett for preparing this blog. You can find out more about Brett here.


